Parlor, pen, rail or headlocks – what works best? Recent research revealed that prevention and control of digital dermatitis (DD) during the raising period positively impacts a heifer’s first-lactation hoof health, reproduction and milk production.
When heifers get infected with DD, we now know they are at greater risk of contracting DD again after entering the lactating herd. These animals also have decreased reproductive performance and milk production during first lactation when compared to heifers kept free of the disease. With the average cost of DD in first lactation estimated at more than $200 per lactation, it pays to focus efforts on prevention and control of DD in heifers during raising.
Don’t use locomotion scoring to identify DD
Locomotion scoring is the dairy industry’s gold standard for identifying lameness. However, when it comes to detecting DD, locomotion scoring actually has limited value. While it may help identify animals with active, painful (M2) lesions with an abnormal gait, this method still misses the proportion of animals that do not have an altered gait yet possess active lesions.
Furthermore, inactive, non-ulcerative lesions (M1, M3 and M4) tend to be non-painful – and thus fail to alter the gait of the animals and further reduce the reliability of locomotion scoring. To effectively prevent and control DD, we need to identify the presence of DD, the lesion stage and chronicity before they develop into active, ulcerative, painful (M2) lesions. Early prevention and prompt treatment are key.
Preferred methods for DD detection
Today, the hoof trimming chute is considered the gold standard location for DD detection. Using a trim chute, DD is easily detected by inspecting each claw, thus allowing assignment of M stages and chronicity scores for each lesion identified. However, it is not realistic for dairies, large or small, to regularly score the entire herd for DD using the trim chute.
That would be extremely time-consuming and expensive. Common alternative locations on the farm that allow more rapid DD detection include the parlor, pen, management rail and headlocks. While all of these locations may be used to some degree of success, which alternative yields the best DD accuracy and predictability?
Zinpro Corporation recently partnered with researchers at the University of Minnesota to investigate this question. Results from the study were presented at the 10th International Conference on Lameness in Ruminants held in Valdivia, Chile.
Study design
Herds from Wisconsin and Minnesota were enrolled for participation according to certain eligibility criteria: use of freestall housing; herringbone, parallel or rotary parlor; regular, professional hoof trimming; and presence of DD on the farm. Prior to the day of hoof trimming, herds were visited to score cows in the parlor, pen (or headlocks, management rail/lane) or hoof trimming chute. In all locations, unwashed feet were examined visually using a flashlight.
All cows were scored by one trained observer. DD status was recorded using the modified 5-point M stage scoring system (M0, M1, M2, M3, M4 and M4.1).
Key research findings
Unfortunately, DD presence was consistently underestimated in the alternative locations. The trim chute (which was used as the benchmark for comparison) had a higher DD detection rate (greater than M0) compared to all alternative locations evaluated (parlor, pen, rail and headlocks).
However, the gap in accuracy for alternative DD detection locations compared to trim chute identification lessened as the lesions progressed into acute and chronic stages (M2 and M4, respectively) and became larger in size (greater than 2 centimeters).
In addition, the accuracy of DD diagnosis was not impacted by the parlor type (herringbone, parallel and rotary). Accuracy of detection in the parlor appeared to be based on the skill of the actual observer, not associated with parlor type.
To test agreement of alternate scoring locations compared to the trim chute, a statistical model was utilized to evaluate agreement between scoring locations. The researchers also evaluated:
-
Sensitivity – the portion of legs truly affected with DD that were properly identified. This indicates how well existing lesions were detected.
- Specificity – the proportion of healthy legs properly identified. This indicates how well feet with no lesions were correctly diagnosed.
The results of this study found that the detection of DD lesions (greater than M0) in headlocks moderately agreed with what was observed in the chute, and as the size of the lesion increased (greater than M1), there was substantial agreement between the two methods. In contrast, the rail and pen locations were less reliable compared to the headlocks.
As observed with headlocks, DD lesion detection (greater than M0) in the parlor showed moderate agreement with the chute, and as the size of the lesion increased (greater than M1), substantial agreement was observed. However, none of the alternate locations were very reliable when it came to accurately identifying specific lesions according to M stage.
When results were evaluated based on sensitivity (Figure 1), none of the alternative scoring locations (headlocks, rail, pen and parlor) were very accurate compared to the trim chute, and they failed to meet the recommended minimum sensitivity score of 80.
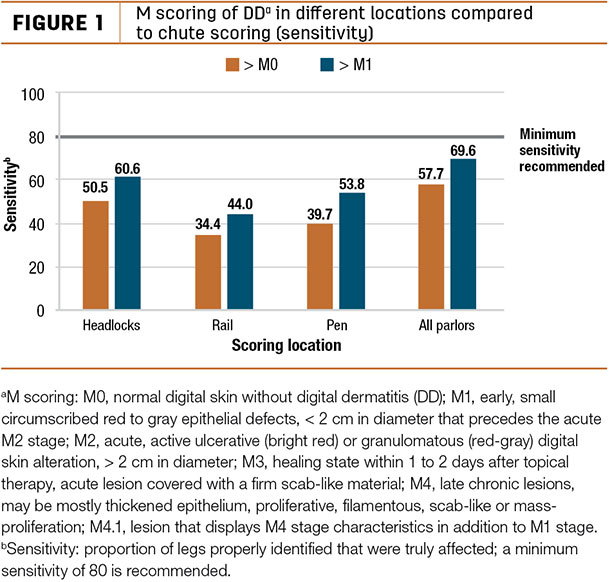
Results indicate headlocks performed better than either the pen or the rail, regardless of lesion stage (greater than M0 or greater than M1).
All parlor types also performed similarly to what was observed in headlocks. In contrast, when evaluating results based on specificity (Figure 2), there was substantial agreement for all alternative locations when each location was compared to the trim chute.
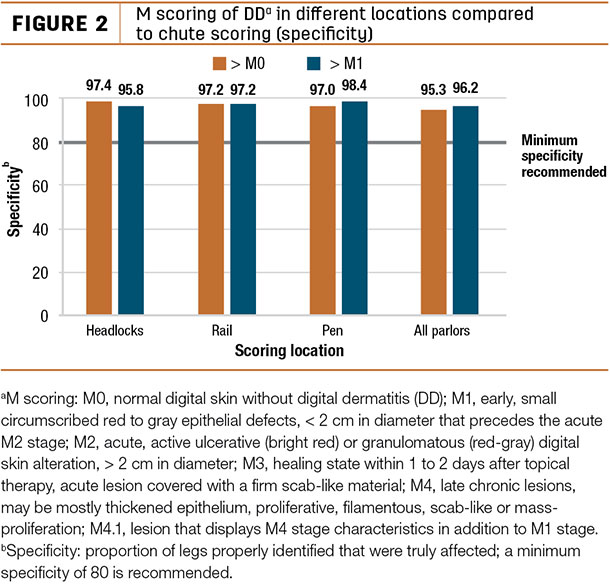
In brief, the results of the sensitivity and specificity tests indicate that scoring in locations outside of the chute may result in underestimating DD incidence rate on the farm, but the occurrence of a false positive diagnosis will be minimal.
The apparent prevalence of lesions greater than M1 in this study is compared to the true prevalence percent. True prevalence of all lesions in alternate locations is being underestimated, and scoring location makes a difference.
Of the alternate scoring locations evaluated, the parlor was the best predictor of true prevalence, followed by headlocks, pen and then rail. It’s important to note that even in the parlor – the best alternate location predictor – the true prevalence is still being underestimated.
With this additional information in mind, we may now have the ability to add an adjustment factor to account for this variation when conducting on-farm assessments. Incorporating a correction factor to adjust for identification failure may allow for more accurate prediction of true DD prevalence on farms. ![]()
Daryl Kleinschmit is a research nutritionist with Zinpro Corporation. Email Daryl Kleinschmit.




