The cost of treating a case of clinical mastitis averages $100 in many dairies and exceeds $200 in some. The use of antibiotics for treating mastitis is responsible for the majority of this cost – not because of the cost of the antibiotics but mainly because of discarded milk.

Then why do we use antibiotics? The answer would be: to kill the bacteria causing the infection. What if there are no bacteria, or the bacteria causing mastitis are not killed by the antibiotics? Do we still need to use antibiotics? Not for more than half of the cases of mastitis. But how do we know which cases need antibiotics and which don’t?
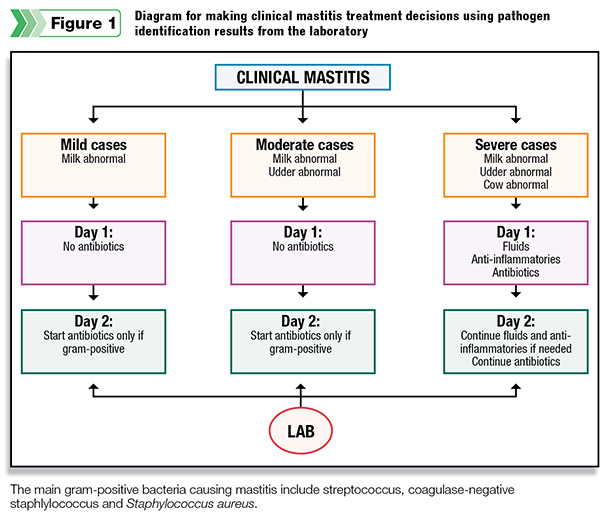
Severity of clinical mastitis cases is classified as mild when only the milk is abnormal (i.e., clots, flakes, watery), moderate when abnormal milk and a swelling udder, and severe when in addition to a bad udder, the cow is sick.
In most dairies, only 10 percent of mastitis cases are severe, needing immediate attention via administering IV fluids, anti-inflammatories and antibiotics. The other 90 percent, mild and moderate cases, are the ones I am going to talk about. Depending on the cause, mastitis cases are classified as:
 • No-growths (no bacteria) – In 25 to 50 percent of the cases of mastitis, there are no bacteria in milk by the time clinical mastitis is detected at the parlor. If there are no bacteria, these cases do not require antibiotic therapy.
• No-growths (no bacteria) – In 25 to 50 percent of the cases of mastitis, there are no bacteria in milk by the time clinical mastitis is detected at the parlor. If there are no bacteria, these cases do not require antibiotic therapy.
The reason for the swelling or abnormal milk but no bacteria is that something else caused the mastitis or that by the time milk is abnormal or swelling appears in a quarter, the cow’s own immune system has already eliminated the infection.
• Gram-negatives – These represent 20 to 40 percent of the cases of mastitis. The majority of the gram-negative bacteria are the coliforms, which include E. coli and Klebsiella. They tend to have a more complex layering in their cell wall structure, which makes it difficult for antibiotics to reach their killing target.
Also, by the time coliform clinical mastitis is detected, the cow’s immune system is already working to fight the bacteria. Most studies have failed to prove the efficacy of antibiotic treatment for these bacteria.
If antibiotics are going to be used to treat coliform mastitis, it is important to select the right one. A recent study showed some efficacy when treating with tubes containing the antibiotic ceftiofur.
However, more research is needed to prove that cows treated with this antibiotic have lower SCC, less chance of being culled or produce more milk after clinical mastitis than non-treated cows.
• Gram-positives – These are isolated from 20 to 40 percent of the cases. The main gram-positive bacteria are streptococcus, coagulase-negative staphylococcus (also known as CNS or staphs) and Staphylococcus aureus .
They really need to be treated with antibiotics if we want to eliminate the infection. All antibiotic tubes available in the U.S. claim efficacy against these pathogens.
Short treatment duration (two or three tubes) is quite effective for most of these bacteria, but not for all. Significantly higher cure rates are obtained for new cases of Staphylococcus aureus and some of the streptococcus when treated for five to eight days.
Management of Staphylococcus aureus cases may depend on the likelihood for cure: Producers may opt to try antibiotic therapy for newer cases but may decide to manage chronic cases differently using such strategies as segregation, drying off the quarter or culling the cow.
• Others – Yeast, pseudomonas, mycoplasma, nocardia and prototheca are not susceptible to antibiotics and are isolated in a smaller percentage of mastitis cases in most dairies.
Now the question is: “How do we know if a type of bacteria is causing mastitis, and if it is, which type of bacteria is causing it?” The short answer is that we do not know without analyzing the milk.
The problem is that milk quality laboratories have not been routinely utilized by many dairies for this purpose because of the several days’ delay between detecting the case of mastitis, submission of milk samples for culture and getting back results from the laboratory.
However, new technologies allow for results back at the dairy in less than 24 hours. But can those one-third to one-half of the cows that need to be treated wait one day without antibiotics? The answer is: yes. There are studies proving that delaying treatment one day does not affect the cure of mastitis or the future SCC or milk production of the cow.
Laboratories need to have daily pick up of milk samples and results sent electronically to the dairy in 24 hours. The process works as follows: The milker detects clinical mastitis at the parlor and collects a milk sample, but the quarter is not treated with antibiotic tubes until results from the laboratory have come in (except in a severe case of mastitis).
Milk samples are picked up daily from the dairy and taken to the laboratory. The laboratory sends results to the dairy within 24 hours. Thus, the next day after mastitis is detected, most dairies make the following decisions with the laboratory results on hand:
1. Not treating with antibiotics cases from which bacteria were not isolated
2. Not treating with antibiotics cases from which gram-negative bacteria were isolated (Some dairies choose to treat these cases with antibiotics that may have some efficacy against them.)
3. Treating gram-positives with two or three tubes of antibiotics (Some dairies treat new cases of Staphylococcus aureus and some of the streptococcus for longer periods of time – five to eight tubes.)
There are also dairies that choose to initiate antibiotic treatment in all cows with mastitis immediately after detection of mastitis and when they receive laboratory results next day.
They stop treatment if bacteria were not isolated or gram-negative bacteria were isolated, or they continue treatment if gram-positives were isolated.
Accurate diagnosis of the bacteria that is causing mastitis is critical for the success of pathogen-based treatment decisions and for mastitis control programs in general. Gram-positives falsely classified as gram-negatives or no-growths will be withheld from antibiotic treatment when it would be beneficial.
Conversely, false gram-positive diagnosis leads to treatment of cases that do not benefit from it. In addition, not identifying contagious pathogens such as mycoplasma, prototheca or Staphylococcus aureus will lead to the spread of infection.
Misclassifying cows as infected with these pathogens when they are not will lead to the culling of healthy cows. Therefore, professional laboratories should be used for bacteria identification.
In summary, not all clinical mastitis cases are equal. Some benefit from antibiotic treatment, but many don’t. Knowing the cause of mastitis allows selecting which cases to treat with antibiotics.
It represents a tremendous opportunity to reduce by more than half the use of antibiotics for the treatment of clinical mastitis without sacrificing the efficacy of treatment or the long-term health and production potential of the cow.
Consequently, dairy herds will incur considerable savings on treatment-related costs (discarded milk, drugs and labor).
Furthermore, knowing the bacteria that is causing mastitis allows adequate antibiotic selection and treatment duration to optimize the cure.
It is important that you work with your veterinarian to develop your clinical mastitis treatment protocols. Finally, rapid and accurate laboratory results are crucial to make pathogen-based treatment decisions. PD
Dr. Alfonso Lago holds a veterinary degree, a Dairy Production Medicine Residency from the University of Wisconsin and a Ph.D. from the University of Minnesota. He is the president of DairyExperts, a consulting management and research firm based in Tulare, California.

Alfonso Lago
Veterinarian
DairyExperts



